Hair loss treatment with a dermatologist
If you have hair thinning or loss, it may be time to talk to a board-certified dermatologist to learn more about your treatment options. At the Center for Dermatology and Dermatologic Surgery in Washington, DC, and Annapolis, Maryland, we can help with restoration solutions for thinning or lost hair.
What is hair loss?
Hair loss and thinning may be related to many situations or conditions. This may include times of increased stress, autoimmune disorders, hormonal changes, or even male or female pattern baldness, known as androgenic alopecia. When our team evaluates you, we can determine the exact cause of your hair loss, which helps us better determine the treatment most appropriate for your unique needs and situation.
How is hair loss treated?
There are several ways to combat hair thinning and loss. This includes certain medications that can be taken, including prescription products and the integration of red lights to stimulate hair follicle growth. We may also counteract hair thinning and loss with topical creams, hormonal regulation, or the use of nutritional supplements. Our board-certified dermatologist and hair technician expert may also consider combining several treatments for faster, more noticeable results.
What is the recovery time for hair loss treatment?
The recovery time when it comes to restoring hair thickness varies depending on the type of treatment chosen.
What is alopecia areata?
Dr. Cheryl Burgess describes alopecia areata as the medical term for hair loss that occurs in small patches throughout the scalp. It often begins with one circular patch that develops as more can with time. It is a result of the immune system attacking the hair follicles, often due to increased stress levels.
Are there risks and complications with alopecia areata medications and treatments?
When discussing your needs, be sure to talk to your doctor about any risks and complications that might come along with thinning hair solutions. They can help you better understand each treatment and make an educated decision regarding which is right for you!
How do I learn more?
If you want to learn more about thinning hair solutions, contact our office to talk to Dr. Cheryl Burgess and her dedicated team.
Our Annapolis, MD office can be reached by calling (410) 224-1195, and our Washington, DC area practice can be reached by calling (202) 955-5757 for an appointment.
We are open to new and current patients in and around these communities and look forward to meeting with you!

The reasons for hair loss, the solutions, and whether they work … find out here!
Hi skin friend. I am so glad you tuned into this week’s episode.
You are in for a real treat because I have board certified dermatologist,
Dr. Cheryl Burgess on with me today.
And we are going to be taking a really deep dive into hair loss.
This is a topic that I find myself talking about all the time.
People are asking me about hair loss, whether men, women, and really anyone 30 and up seems to have at some point in their life experienced some sort of hair loss and it can be really, really traumatic.
And so people have a lot of questions about it.
There’s a lot of information out there, a lot of companies, a lot of products, and it’s kind of hard to know, well, what’s real? What’s truth?
What’s going to help me? What’s not, what should I spend my money on?
And I love that Dr. Burgess is sharing with us some really great tips and perhaps some information you didn’t know about with some common supplements that actually can really, really help with hair loss.
Dr. Burgess is the founder of the Center for Dermatology and Dermatologic Surgery in Washington DC. She’s a medical expert, key opinion leader in the field of dermatology, and she’s really going to be sharing some great pearls with us today.
So I am so glad you tuned in. Let’s get started. Dr. Burgess, thanks so much for being here.
It’s wonderful to have another dermatologist on and someone who has a lot of knowledge and expertise with hair loss.
So thank you so much for being here. Thank you for having me.
I heard a lot about your podcasts and I’m excited to contribute to it today. Well, you know what?
It’s a lot of fun doing this because A,
I love talking about skin and skin conditions as I know you do too, and educating people and putting really good information out there.
And it’s also a great way to connect with my colleagues.
It’s a lot of fun to meet all these wonderful dermatologists as well.
So that’s another little perk about the job that I enjoy too. Well, I definitely want to jump into today’s topic, which is hair loss.
And I’ve already had some episodes on hair loss, but I find this is a topic that never gets old.
I am always asked about it. What about you? Always, it’s kind of the running joke that you don’t want a hair loss case at four o’clock on a Friday because you really get involved in it and you’ll be there to six o’clock. It can be emotional, it can be tears of joy when people find out that their hair loss is not permanent.
And so it goes through the spectrum.
And so you really need to spend time with a patient with hair loss in order to discern if they have one or two or maybe even three types of hair loss going on at the same time, over 20 types of hair losses that people could have.
This is not a quick in and out visit, especially for the first visit.
And not only do you want to see if there is an underlying medical condition, but there is so much psychological impact to the hair loss that has to be addressed as well. And this isn’t just for men.
This is an issue for women and men with hair loss. It can really, really be traumatic and distressing for people.
So totally great point.
It’s not a quick visit and I love that you bring up there 20 kinds of hair loss or more than 20 kinds of hair loss because a lot of times people just, I think they think about well balding in men and maybe balding in women and that’s it.
But there actually are so many different kinds of hair loss.
Can you just walk us through what’s your approach when you have that patient come in, hopefully not at four o’clock on Friday with hair loss?
What’s your approach? Well, first of all, when people call on the phone that they have hair loss, I always have them come in because hair breakage is different from hair loss and sometimes it’s just the physical products and styling methods that people have and that they do that will cause breakage of the hair. So that’s the first thing I need to determine.
Are we truly losing hair by the root or this is just breakage?
And so that’s the first thing. Second thing is if it is truly hair loss, I’m going to do some tests to try to find out if there’s a medical reason or this could be a temporary issue.
There’s a condition that we see commonly, I know you probably do as well, that we see in pregnancy and after pregnancy when women deliver their babies about three months later, they have a shedding of their hair, which is called telogen lium.
So I can usually predict the age of the baby.
You have a three month old, right?
And so those are situations in where we find that it’s more of a reactionary hair loss versus a permanent hair loss.
And then we have to define is it a scarring hair loss, which we have to intervene a little bit quicker than say the other types.
So there’s so many different routes and pathways we can go with just the history of getting that information from the patient.
And that takes time. Like you were saying, this is not a rushed visit and there are not many dermatologists in the country who even dress hair because it is long and detailed.
So the first thing you want to find is a dermatologist who deals with hair. It’s so multifactorial what could be causing it. And you’re so right.
You got to see the patient too. You got to see what you’re dealing with, see what their hair looks like, what their scalp looks like. Is it breakage?
What hairstyle are they wearing? What do they do to their hair each day?
Are they pulling it back really tight?
We were talking briefly before we started recording right about how I was talking with my staff about it that some of them were saying they felt like they were getting, they didn’t want to pull their hair back for surgery because they felt like it was going to cause their hair to break and they were going to get some traction alopecia, which is from the pulling and the tightness.
And also I feel like even as I’m getting older, I’m noticing some hair thinning of my eyebrows, a little hair thinning around my temples.
And even though people looking at me are like, what are you talking about?
I don’t see it when it’s happening to you. Right, you see it and it can be bothersome. Exactly.
Because some people with very thick coarse hair will come in and say, the first thing they say is, I know you think I’m crazy, but I am really losing my hair. I had way more hair. And I’m like, no, I believe that you’re telling the truth. So let’s try to get to the bottom of it.
So it doesn’t matter if you initially started out with coarse hair or fine hair and people have different patterns of hair, we kind of graded into one through four, sometimes five, depending on the nature of the hair.
And we first have to classify you and diagnose you and determine there’s some scalp issues. Is it just the shaft of the hair issue?
Is it the root issue? Is it just breaking at the end? And unfortunately, there are a lot of people who think hair grows from the tip from the end, and so just going through the anatomical features of hair and educating people is very important.
Totally agree with all of that. And you know what interesting, we talked about telogen effluvium with pregnancy, with yes, I have experienced that with both my children and my friends have, and I see it in that age range and certainly a couple months, three to six months after delivery, but I’ve actually seen it a lot after people have had COVID.
Have you noticed that? Oh, yes.
It was big time and telogen of flu.
I tell patients it’s more of a reactionary type of hair loss and it’s not something that happened last weekend or the weekend before. It’s something that happened three to four, maybe even six months prior.
And so it’s more of a shock to your system.
Something like COVID was a shock to our system.
It was something new just like the passing of a relative or a spouse or something.
There are different things that can elicit a traumatic event at the hair root level and it pushes that hair through the cycles much sooner than it would normally be. So when people come in with a telogen flu, I have to go through the history and say any illnesses, any surgeries, any anesthesia, any stress to your system, which is very important because I have them backtrack.
And when did you really see all this shedding?
Typically they’ll say Hair was all over my clothes on my shoulders, all on the sink, on the floor in the shower after I shampooed my hair.
And I’m like, well, when did you kind of notice that? And they may say, okay, October this month, then I’m going to backtrack and ask them at least maybe four to six months ago.
Was there anything that was going on during that time period?
I’ve seen it with covid. I’ve seen it with the covid vaccines.
I’ve seen it again, like I was saying with surgery, anesthesia, medications, change in medications, maybe a dose was changed.
And then sometimes we can’t figure it out.
People go home and they come back and let you know what I was thinking about it, and I realize it was this.
And generally if I can cut a tag when the stressor occurred or with the stimulation of that phase of early quick cycle from antigen to telogen, then I can almost tell them when it’s going to stop.
And usually we see it stop about a year after the initial insult.
So most people who come to you are six to nine months into it anyway,
and so it’s few months later that they have to deal with it.
And to convince people, I have them do a hair collection test.
I have them take all the hair that they have for the day that they pulled out or brushed out or combed out, shampooed out, put it in a baggie and label it the day of the week and the date.
And then we have them do it for 30 days and we line it up like a calendar.
So physically you can see that it’s getting less and less.
Sometimes you have to be able to show that if it’s not, we can somewhat calculate that it’s going to last a little bit longer, but it tends to slow down and you can see that happen.
So that’s very helpful for patients because they get distraught about the hair that they’re losing. And for the most part, if they don’t comb their hair today, it’s twice as much tomorrow and three times as much in the third day.
And they don’t realize that not combing their hair is going to save the hair from falling out because it’s in that telogen phase.
So it helps people also comb their hair every day so that we can do the hair collection in the baggies and telogen filium, you can actually see it slow down.
Now there are some treatments that I do for that to kind of speed it up and what happens, I usually ask people, well, how are you sleeping at night?
And yeah, I’m just stressed that don’t sleep at night. Well, melatonin at three milligrams each night.
Taking it at night tends to help to slow down that telogen of flu.
So that’s what I normally put patients on and generally within a month it’s really slowed down.
So that’s one of my vices to people who undergo a stressful telogen flum type of event. I love that hack. I didn’t know that, but I’m writing that down. I’m going to try that out. I love that. Yeah, it’s really helpful.
And it probably also helps with sleep and a lot of people
are taking it anyway, so if it can help. So melatonin comes in 1, 3 5 and 10 milligram pills.
Some people can take too much and they don’t see anything occurring.
I find it works best with the three milligram just at night gets the circadian rhythm back on par and they start to see a difference in the machete. That’s a great little pearl there, so I love that.
Thanks for sharing that. And a lot to unpack there about telogen effluvium.
I know some people think, well, it’s reversible, right? It’s going to go away.
You’re not going to be left with bald patches, so why do you even need to treat it? And that’s a fair valid point.
You don’t have to treat it, but if you can speed it along, help it along, that is helpful for the person going through it because it is distressing.
And then you see all those little hairs growing back and if you can hurry that along, it is helpful. So I love that.
And I find that a lot of patients don’t associate the stressful event with their hair loss.
There just seems to be too much time in between that it’s hard to think back.
Something that happened three months ago, five months ago, six months ago is causing my hair loss today.
That’s hard to have people wrap their heads around, but it’s true.
But that is good to know. Yes, it’s temporary, it is going to come back and now we’ve got a nice little hack for speeding it along with melatonin, so that’s great.
And I also like your idea of having the patients collect the hair.
I find that a lot of times they’re already collecting it anyway, or at least after a shower they sort of ball it up.
I know I would look at it and think, oh my goodness.
And so if you can have them collect that and then they have this visual cue of how at the first of the month it’s here and then it’s diminished rather than putting it all in a bag, they’ll put it all in a bag and bring it to you, but you can’t really assess roughly a hundred hairs when it’s all gathered like that. And so I can typically, depending on the length of the hair, determine if this is a hundred hairs or not, and over a hundred hairs a day puts you in that category of telogen flu.
But also I’m assessing and looking, is this breakage or are the roots?
And you can also, as a dermatologist, we can look under a microscope and see the telogen bulb on the hair so you know that we’re in the telogen phase versus an antigen phase. So I try to go through all of that.
It’s really funny that most people who come want you to do something to help their hair grow back quicker.
And if you don’t, they tend to feel that you weren’t listening or you didn’t do a good job. But there’s certain hair loss situations in where we have to give it time and have to watch the pattern and have to treat it accordingly.
There may be labs and biopsies and things we may need to do prior to.
So not all the time do we give them something to treat the hair loss with on the first visit.
And with hair loss and really with so much of what we do in dermatology, it takes time. But I feel like especially with hair loss, there’s not a quick fix. It takes time. Now let’s kind of segue, you were mentioning labs and biopsies, things like that.
When do you find that you need to do those kind of procedures? Well, what I find you could have a medical condition that can lead to telogen.
Therefore now we’re looking at two types of hair loss.
And so that’s why it’s important to really get a history from a patient that may not be the only thing that’s going on. Like I said, there’s stressors and different things that cause the telogen flu.
So I’m going to look more in depth to what possibly could this be.
I’m going to draw labs on patients.
I’m going to possibly do a scalp biopsy in the hormonal area and the non-hormonal area in which it requires two biopsies on the scalp, it’s pretty universal that if you’re doing a biopsy on the scalp, they’re four millimeter punches.
And I find that people will bring in lab reports where they’ve had a biopsy before and it was a two millimeter or a three millimeter, and therefore, so I’m going to assess their labs and any previous biopsy that they’ve had to determine if I really need to biopsy if it was adequate.
Sometimes I’ll get their previous labs, get that fended for a second opinion at my lab, so they kind of forego another biopsy.
So there’s a lot of things that we can do to speed things along for patients, but if it’s been a few years,
I’m probably going to re-biopsy it because things can change during that length of time. And for the most part, it could be a different type of hair loss.
So it’s really important to totally assess a patient.
But like I was saying, the labs are one thing that I’m going to look at.
I’m going to do a hair pull test and look how easily I can pull the hair out of the scalp.
I’m probably going to do some labs and depending on it’s a male or female, depends on the labs that I’m going to draw.
But I’m looking at a lot of different things in the labs.
You could be anemic, you could be iron deficient.
There are so many things that you may not even know when you come into the office that you feel healthy and nothing’s wrong, but I may find something on your labs that’s abnormal and we can correct in some of my patients, it’s the vitamin D level that’s really, really low and they don’t even know it.
Especially in my black population, they naturally have very low vitamin D levels.
So I’m going to check all of those issues.
And if it’s a premenopausal woman, I’m going to check for maybe polycystic ovarian syndrome, other medical issues that could be causing them to thin like female pattern baldness and also have a telogen and flu.
So that’s what I’m going to look at.
I’ve been hearing a lot and reading a lot about vitamin D and how that surprisingly is low in a lot of people and it’s typically people with darker skin who are unable to metabolize the vitamin D in their skin.
And so a lot of times you don’t recognize that until you get that blood work and that I actually just recently broke my fibula, and so I’ve been seeing the orthopedic surgeon and he was telling me I should be taking 2000 milligrams of vitamin D.
And so it just seems like we’re learning more and more about vitamin D and that maybe we need to be supplementing a little bit more than we previously thought.
And I know I practice very strict sun protection, so I probably am deficient. Yes, a dermatologist, we advocate that and people were like, well, I need the sun.
We do need the sun.
So we’re kind of stuck between a rock and a hard place because yeah, it can be an issue in certain situations still.
And I think you’d agree with me, just supplement with vitamin D, don’t go to the tanning bed, don’t go out and get a sunburn.
And a lot of times the people who are vitamin D deficient tend to be people who have more melanin in their skin to begin with.
And so if you are someone more of my complexion light, you go out and get sunburned, you’re really not helping your vitamin D.
You’re really just helping yourself develop skin cancer are most likely.
What about biotin? Do you ever check for biotin levels or, I know in the past people used to recommend biotin for hair loss and now we’ve moved away from that. I don’t check it. I do.
You do? Okay. I love it. I want to hear, you know what?
Because what I find is people are ODing on biotin.
I check their levels and they’re so high. I’m like, stop it. Stop the biotin. We find, and I agree with you, that is not a solution for hair loss.
I’ve seen it help nails, but for hair I find vitamin D supplementation is so much better than biotin and I have to show patients, look at your biotin level and look that you’re still having these issues.
So just stop. Just stop the biotin. But yeah, I do it for that reason.
What do you recommend for vitamin D supplementation? Now I’m curious, do you recommend 2,005,000 or do you base it off of how low they are? Well, if a person is under 30 milligrams per deciliter, I pretty much will recommend the ergocalciferol, which is 50,000 units just weekly.
And if you look at it taking 5,000 every day, you could still do that.
But some people are on a lot of different medications and they’re like, can you make it simpler for me? And that’s what I do.
I just give them the prescription. But you could take 5,000 a day and be adequate.
Now keep in mind though, it does take a while to get that vitamin D level up. And if you’re at 20 and you’ve taken 50,000 international units weekly, sometimes three months, it inched it up maybe three notches or four notches.
It doesn’t do it very fast. And so I tell people, I may be doing this for six months, but let’s see how you do.
And one thing that I tell patients is that because a hair cycle works on a three month cycle, this gives something to hair cycles to work or not work.
Okay. I don’t keep people on things a long time.
So if you think you see something going on in three months, we’ll continue it for six months. At six months.
If I don’t see anything going on, I know it’s time for me to change my methods or direction in where we’re going with the hair. So that is one thing.
It’s not you have to do something for years and years and years to correct your hair. You kind of know if it’s going to happen within six months, but you do have to give it those six months. Right.
And I want to correct myself. I was saying milligrams, but you’re right.
It’s international units for the dose for the vitamin D. No, you had it right. So well beyond vitamin D, which again, I’m kind of becoming a big fan of for my bones and for my hair.
Do you recommend supplements routinely for hair loss? We’re seeing a lot of ’em.
Yes. I do. Years ago, because I was really doing a lot of hair including hair transplants and things like that, and I got to the point where I saw that a lot of the hair loss that came to me were gender specific, mainly females.
And that the females didn’t need hair transplants. They were fine.
They just wanted to stop shedding and be able to style their hair.
And so I let all the hair transplants and things go to Bosley because they do a better job at volume than I could do in my office.
But I found that most of the conditions were medical and they were not addressing that in women.
And so that’s how I got into, there’s a product called Viviscal, which came out in the late 1990s, and it has really evolved since then because there’s now the original formulation and then there was an extra strength formulation, and now we have available in our offices the professional strength. And shortly after that, maybe about 10 years ago, then Neutrophil came out and they have a whole line of products.
And both of these hair supplements are very rich in vitamin D.
So sometimes you don’t have to supplement if you’re taking those products.
Some of them have shellfish or mollus origin, shark origin, but it’s definitely marine and the marine substances are very high in vitamin D.
I remember my grandmother telling me we have to have fish every week because fish is brain food. And that was true.
Vitamin D was very, very necessary for our bones and our brain and everything else.
And so it’s still to this day is very helpful with a lot of different conditions.
So you’re getting a high source of vitamin D in those nutraceuticals. Yeah, I know a lot of people who have used both of those products and have found them really helpful. But it’s interesting.
I wonder maybe if you also just supplemented vitamin D, perhaps you could see a lot of those changes too. So it’s interesting. You can, so physicians who don’t carry products in their office, yeah, I mean I go anywhere from the nutraceuticals to the prescription ergocalciferol 50,000 a week to just go over the counter. It just depends on what people want to spend on.
Some of the nutraceuticals can be expensive, but it doesn’t have to be in order to increase your vitamin D level.
Now let’s talk about some of the other medicines that we can use for hair loss.
So I think it was a New York Times article a couple years ago about low dose minoxidil, and I’m sure in your office too, we just had tons of people coming in asking about it.
Tons is an understatement, right? Tons. Well, yeah, it’s an understatement.
But you know what?
It’s really funny because I remember in the late 1980s, you probably weren’t born then, but I was finishing my residency and we were taking the NAL pills, grinding them up, putting in propylene glycol and rubbing it on our heads.
And then that led to the research and the FDA clearance for RO a, which was the 2% that initially came out.
And then later on the 5% came out.
Now we’ve kind of reversed course and gotten back to that pill.
So we’ve gotten back to Minoxidil as a pill and it would gangbusters when it was published in New York Times and Washington Post about how it can grow hair.
Our office was inundated with calls and so I’m sure every other dermatologist and I’m like, wow.
So we’re kind of reversing and going back to what we found was really helpful.
And so I do see a great improvement with that, better than topical. So I have a lot of people on it now.
I start women at a lower dose than I start men and then gradually increase them.
One of the side effects could be lowering of the blood pressure because it is a blood pressure medication, but those who are already on antihypertensives, I have them clear it through their internists or the person who’s prescribing the antihypertensive to them and see if there’s a way we can juggle it where they can be on both.
But it’s such a low dose at 2.5 milligrams, and I think for a more medical dose, it’s greater than 10 or 10 milligrams.
And so we’re at a fraction of that dose.
One of the side effects that I always tell patients, and I’ve never seen it happen, knock on wood, is that they can have a little bit of lowering of their blood pressure within the first two weeks of taking the preparation and within the first two hours of swallowing the pill.
And what we find is that that tends to go away.
It’s not a reason for them to stop the medication.
They may have, I was saying a little orthostatic hypotension for a second.
You kneel down to tie your shoelaces up, but it’s not anything in where people are passing out or anything like that.
So we find that it’s very safe and some people, we see a little bit of hair growth around here and on the face, but again, people are like, well, I just shave it off and you can shave it off and shaving the hair off doesn’t bring more hair follicles. So most people think, yes, let’s squash that. Let squash that wives feel. Yeah, a lot of times when Roane first came out, people would see that and they thought it was media absorption along the hairline, but once you kind of shaved it off with some of those little fine dural plane blades, it doesn’t come back.
Sometimes You never know, but it’s so fine and baby like that, you could remove it easily.
I just saw a lady today who had very, very thin hair.
She had gone through menopause and really lost a lot of hair and had thin hair, and we put her on minoxidil and I just saw her back. It’s been about a year now, and she is just loving it.
I asked her about if she had excess hair elsewhere on her face or her body that was bothersome, and she said, well, she could maybe notice a little bit. She said, it doesn’t bother me at all.
She’s just so excited to have a thick head of hair. That side effect, it really is minimal. And most of the women are like, look, I’ll take a little bit of that baby fuzz to get a thicker ponytail and thicker hair. Well, and as you get older, you get that peach fuzz on your face anyway, so it’s not that different than that.
And we shave that peach fuzz. I know.
Why does extra hair grow on places you don’t want it as you get older and you’d lose it in a place? I don’t know. I don’t know why the ears grow.
Men get it in the ears and the nose and women get mustache and beard and its little whiskers. Yeah, exactly. Yeah, but that’s okay.
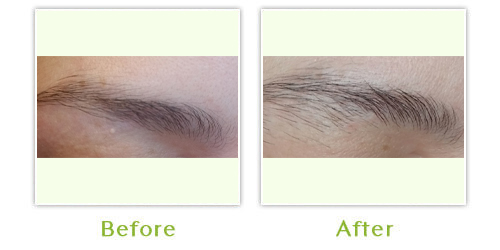
You just pluck ’em and move on. That’s right. Well, I am a big fan of the minoxidil and the topical preparation for people who don’t want to do the oral version. I find it works great for eyebrows.
People notice their eyebrows are getting sparse.
You could put a little bit on or your temples, you could rub a little bit on wherever you feel like your hair is thinning.
But yeah, I think if it’s more widespread and you just have overall thin hair, then the oral minoxidil is a great option for a lot of people.
It really is. And safe. Yes, very safe. Yes. We’re talking very, very low doses for sure. Now what about any in-office procedures?
Previously you did hair transplants, right? Yeah, I do a lot of platelet rich plasma injections or PRP and a lot of people have heard about it.
The unfortunate thing, sometimes it gets a bad rep because there are people out there doing it and don’t really understand how the pathophysiology of what we’re really doing, and sometimes they’re just injecting.
I will get patients who have had five courses and they’re like, I haven’t seen anything. I’m like, okay, something’s wrong here because you should see something in my patients.
I see growth within a month if you’re doing it correctly.
So one, as a dermatologist, we’re used to injecting.
We know how far down the hair follicle is, which is like four millimeters, and we’re not going to float the PRP and fat where there are no follicles.
And I think that’s what’s happening in a lot of these places that are opening up just trying to do PRP.
There’s a science to what we’re doing.
There are stem cells and growth factors that we’re trying to stimulate the hair follicle and we need it near the hair follicle and not away from the hair follicle. And if it’s done correctly, I find when I bring patients back in four to six weeks, I see growth. I see density starting.
And so that’s how I do it. What I do, I look at them like in three months basically because what is the purpose of doing it every month?
None of that science has been worked out.
And why are we injecting every month when a hair cycle is pretty much three months?
We see that people are signing up for four to six treatments every month and nothing’s happening.
So there’s something wrong.
And I don’t think that this will ever be FDA controlled or cleared in a way because we’re looking at drawing the person’s blood.
Their platelet level may be different today than it is next week. Different. Mine is going to be different from yours.
What’s the difference or what’s the criteria that we need in order to know what’s successful and what’s not?
We’ll never know that because we all are different and I wouldn’t use my blood serum on you and you wouldn’t use yours on me. So we’ll never know that data.
And the FDA cannot control that aspect.
So it’s really kind of willy-nilly out there, people doing it.
And there’s no safe science that they’re doing, no safe procedures that they’re doing.
Some people are using big needles and some people are using small needles and there’s no system to what is being done.
And it’s kind of giving it a bad name. But I inject the scalp, I inject eyebrows. I inject just only temples if the temples are thinning out on people.
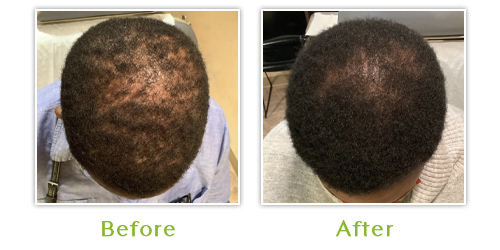
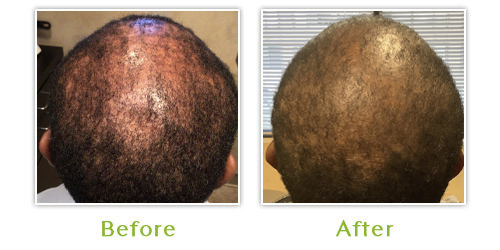
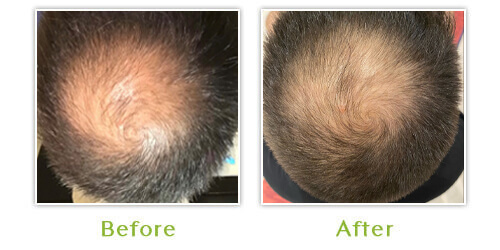
And I post my before and afters on Instagram, and I use social media for my before and afters, and patients will give me permission to show their before and after photo because they’re really proud of that. It worked. And a lot of them are one time.
And if you see someone who was doing it, you ask for their before and afters and you ask, well, what was the timeframe in which this person took the before photo and the after photo?
It’s very important if you’re going somewhere for six months and seven months, like I said, after six months, I know something’s not working.
Just from the pathophysiology of how hair works, it’s such a great point that you got to know who’s injecting it, what their credentials are. It may sound like, oh, so simple.
You just stick a needle into the scalp, but there’s more precision to it than what may seem like on the surface.
And yeah, if you’re not getting the results because it should work, it’s shown scientifically to work, something else is going on. And again, you have to question, well, how’s it being done? Who’s treating me?
And is this really, maybe there’s something underlying going on causing the hair loss, which again is why having an expert like a dermatologist evaluating you is going to really be impactful.
Do you ever do microneedling on the scalp to help stimulate either doing the PRP or alone?
Well, I actually use 30 gauge needles to inject at the level of the follicle. I’m not a big fan of the Microneedling, just roughing up the scalp to put topical PRP to rub it on. I feel the follicle is much lower than that, and it’s much deeper.
And we’re talking about 1.8 millimeters down.
You’re really to the epidermis basically and upper dermis.
So we know measurements of how far the width of a epidermis and the width of a dermis and where we really need to be.
And so looking gauging the needle to where we need to be.
You’re not like Hitbone.
So some of my patients would come in and say, yeah, I could hear hit the bone. Oh my. I’m like, oh my god.
Oh boy. That was deep. That was deep. My goodness. Wow.
Well, gosh, I could talk with you for hours I feel like about hair loss.
This has been awesome, but I want to be respectful of your time, but can you just leave us with three tips for, let’s say a woman who’s noticing hair loss.
What are just some three tips she should do or be thinking about? Well, one most common,
I always say there are more forces out there than zebras.
Okay. And it’s going to be probably something common.
And just don’t stress yourself over it before you see a qualified dermatologist who specializes in hair. Even though we all go through our residency and we learn skin, hair, and nails, there are a lot of dermatologists who don’t want to see hair, just like there are a lot of dermatologists who don’t want to see nails.
They only want to see skin, and that’s their prerogative.
So be aware that there’s certain people who just don’t want to see hair loss cases and to go to someone who’s going to spend the time with you and try to figure out what’s going on and not just have you leave out the office with roe, that’s very typical. I see that all the time.
So be more cautious to who you go to see for your evaluation. So that’s one tip.
Most of the hair loss are going to be very more horses than Z where they’re going to be the more common ones like telogen, lium, yes, you could have some female or male pattern baldness, but we just discussed there’s so many good things out there for this and you nip it in the bud right away. You might have to stay on it for a while, but for the most part we can well, that exaggeration of thinning that we can see in men and women. And thirdly, be patient with the hair growth situation because hair can grow on the average of centimeter a month, so roughly 10 to 12 centimeters a year.
And if it’s breaking faster, the things that you’re doing, and I always discuss that with my women, particularly if you’re dying your hair and bleaching your hair and doing all this and it’s breaking as fast as it’s growing. Yes, it’s going to seem like it’s taking a long time.
So hair has cycles and it grows a certain length, and you have a hundred thousand hairs on your head, and you’re not even in a tale of flum situation, you’re not going to lose all your hair because you have to remember there’s an antigen hair or growth hair pushing that hair out.
So it’s really not a hair loss situation.
There’s a hair that’s pushing it out, trying to grow in.
It’s just the processes moving pretty quickly.
And if we think about that, and then I was saying that there are medical conditions like folliculitis of the scalp or lupus of the scalp, and just other things that we would dive more deeply into.
Again, that’s going to take some time as well.
But I realized being a woman that that’s the most traumatic event that can happen.
I’ve had a telogen of flu before when I was on a medication and I know better and I’m freaking out like, wait a minute, this is like now.
And I calmed myself down and said, it’s got to be okay.
And it was okay. So in most instances, it’s going to be okay. So it’s just figuring it out.
And occasionally we do have the zebras who come through, and then that’s when I put my thinking cap on and I remember my medicine and we go for it because we have to also remember our internal medicine.
And that is going to help us figure out if there’s some medical issue and why the person is shedding their hair or losing their hair.
All great tips. And this has really been super educational for me, and I know the audience, Dr. Burgess,
if people want to come see you in your practice or follow you on social media, where can they do that?
So our social media handle where they can look at some before and after hair loss is C as in Charles, T as in Tom, R as in Robert, the number four dermatology.
And I’ll leave that in the show notes. Okay.
And our website is CTR, the number four dermatology.com.
That’s our website.
And I am in Washington DC and probably close to a lot of places on the East coast, I’ll put it that way. Well, wonderful. Well, I really appreciate you being here and sharing all your expertise about hair loss.
And I didn’t realize we have you to thank for some of those early trials for roane.
So thanks a lot for that. That’s wonderful. Well, thank you so much and we’ll see everyone next week.

PRP treatment at the Center for Dermatology and Dermatologic Surgery
I’m Dr. Cheryl Burgess, board-certified dermatologist in Washington, DC. I am the co-founder and owner of Center for Dermatology and Dermatologic Surgery. I’m going to talk about PRP. There’s a lot of interest in platelet rich plasma, and what does that mean? That is a procedure that has been used for many, many years in other specialties of medicine, but in dermatology we find that people are inquiring about this PRP technique for hair growth. It is used to stimulate hair growth in male and female pattern baldness and other types of alopecias.
This is a technique in where the patient comes to the office, the blood is drawn, the blood is then spun down so that we can harvest the growth factors and stem cells of the patient and then we re-inject those stem cells and growth factors into the scalp, or the area of where the the hair growth is needed. And so this is a technique, it’s not a new technique, but it’s gotten a lot of press by a lot of people doing it. I advise people who have issues of hair loss to consult with a dermatologist who specializes in hair loss.
Although all dermatologists get hair loss and hair growth issues and training in their residency, not all pursue that in their private practice or once they get out of residency. It’s really important that people understand the growth patterns and the cycles of hair growth in order to really evaluate if they’re responding to the PRP. In my office you should see a result or some hair growth within one month. We do see that with our patients, if it’s done correctly. If you’re interested, I would contact the Center for Dermatology and Dermatologic Surgery and call for an appointment.

Hair Loss explained by Dr. Cheryl Burgess
When patients come to see me for hair loss, what I try to explain to them is there are a multitude of reasons why people lose their hair. It’s not always female pattern hair loss. I think that’s what scares most women when they start shedding.
But there’s a number of reasons and there are a number of causes. But the thing is that most of these come about three months prior to the person coming into the dermatologist’s office. So that’s one thing I do want to specifically point out.
People think it was something they did the weekend before or because they just got their hair colored or chemically processed; that’s what’s happening. So when we look at hair loss, we look at, are you losing it from the root? Or is it breaking? Are there fractured hairs? and then we determine which one it is and go from there.
If it is a hair loss situation, we try to determine whether it is a scarring type of hair loss or a non-scarring type of hair loss situation. So when patients come in and say I have alopecia or I was told I had alopecia, well, alopecia just means hair loss. So it’s very important to get a diagnosis of what type of alopecia that you have.
Therefore to do that, the dermatologist comes in. Sometimes it requires blood work and sometimes it requires a scalp biopsy to determine what’s going on at the follicular or root level. Occasionally we will see infections of the scalp, like a fungus infection or a folliculitis or bacterial infection that’s causing you to shed your hair.
So it’s very, very important to consult with the dermatologist when you have hair loss and we can take it from there and do a workup. I know in my baseline workup, I am looking at hormones and looking at your thyroid. I’m also examining the hair under the microscope to see am I dealing with just breakage because you wear your hair bleach blonde and that really strips the Keratin or strips the protein of the hair.
Unfortunately, dermatologists are trained in skin, hair and nails, but they’re not a lot around who’s specifically trained and do further training and specialized in hair loss. So even with dermatologists, you do want to choose someone who is accustomed to dealing with that on a daily basis.
FAQs – Hair loss treatment
If you notice a receding hairline or areas of thinning hair, you might be struggling with hair loss. Our board-certified dermatologist at the Center for Dermatology and Dermatological Surgery in Washington, DC, and Annapolis, Maryland, will be able to provide a thorough and definitive diagnosis while ensuring proper treatment based on the type and severity of your condition.
Absolutely! Dr. Cheryl Burgess can provide a specific diagnosis regarding the type of hair thinning and loss you are experiencing and then develop a unique treatment plan that works. We invite patients to talk to the doctor about all available options and decide on the most appropriate treatment. Some treatment options available at our office include red light therapy and oral and topical prescription medications to stimulate hair growth and thickness.
To learn more about Alopecia Areata, please click to read the Alopecia Areata Study posted on our website, the Center for Dermatology and Dermatologic Surgery.

Make this the month you start loving your hair again
The Center for Dermatology and Dermatologic Surgery Center is a key site for Clinical Research Studies and Dr. Burgess is a principal investigator for clinical trials in medical and cosmetic dermatology. Keeping abreast of the latest medical and cosmetic developments provides our patients with the most updated information.Annapolis ; Washington .